
Antibacterial Drugs
last authored: Feb 2010, David LaPierre
last reviewed:
Introduction

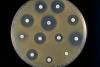
antibiotic sensitivity and resistance
image courtesy of CDC
{kind=link}
There are many drugs available to treat bacterial infections, with different drug types best suited for treating specific infections.
The first determination is whether or not the patient has a bacterial infection. If clincial suspicion is low, and if the patient's condition is stable, deferring or avoiding the use of antibiotics until diagnosis is made is very important to prevent antibiotic resistance. However, if a patient's condition is serious, or in infections where bacterial pathogens are likely (UTI, pneumonia, etc), emperic therapy can also be used.
Factors which influence antiobiotic choice include bacteriostatic vs bacteriocidal action, the need for concentration-dependent (infequent, high doses), or time-dependent (more regular dosing) action.
On occasion, the patient does not improve after starting antibiotic therapy. Reasons for treatment failure to consider include:
- wrong diagnosis
- inadequate activity at site of infection
- antibiotic resistance
- impaired immune function
- undrained source of infections
The following describes the various classes of antiobiotics and their members.
Cell Wall Inhibitors
- penicillins
- cephalosporins
- carbapenems
- glycopeptides
Penicillins bind to penicillin binding proteins (PBPs) with bacteria, leading to distorted cell walls and lysis.
drugs |
coverage |
indications |
adverse effects |
benzyl penicillin
|
NOT
|
mild-to-moderate infections:
|
|
aminopenicillin
|
NOT
|
often used in combination with gentamycin (gram -ve) and clavulin (for a boost) |
|
isoxozoyl penicillin
|
|
|
|
ureidopenicillin
|
|
|
|
lactamase inhibitors
|
|
|
|
carboxypenicillin
|
|
Beta-lactam resistance has evolved in a number of ways. These include:
- production of beta-lactamase
- altered PBP (S. pneumoniae)
- new PBP (MRSA)
- altered permeability (not as important)
Cephalosporins bind to penicillin binding proteins (PBPs) and prevent cross-linking of peptidoglycans, leading to distorted cell walls and lysis. They are beta-lactams.
- inhibits PBPs, preventing cell wall synthesis
- more resistant to beta-lactamase than penicillins
drugs |
coverage |
indications |
adverse effects |
1st generation
|
gram-positives +++ NOT
gram negatives
|
|
|
2nd generation
|
gram positives ++
gram negatives ++
|
|
|
3rd generation
|
gram positive +++
gram negative +
|
|
|
4th generation
|
gram positive +++
gram negative +++
|
|
Carbapenems bind to penicillin binding proteins (PBPs) and prevent cross-linking of peptidoglycans, leading to distorted cell walls and lysis.
drugs |
coverage |
indications |
adverse effects |
imipenem
|
gram-positives NOT
gram-negatives
|
|
|
meropenem |
Other agents include ertepenem and dorapenem.
Glycopeptides bind to D-ala in nascent cell wall peptides, preventing cross-linking during peptidoglycan formation. Glycopeptide resistance can be a problem in S. aureus and Enterococcus. It occurs via an altered target: D-lac in place of D-ala.
vancomycin
Renally dosed; AUC/MIC-dependent killing.
coverage |
indications |
adverse effects |
gram-positives
not:
|
severe, life-threatening gram-positive infections
antibiotic-associated pseudomembranous colitis caused by C. difficle (oral administration)
|
|
teicoplanin
- gram-positives, including MRSA
- NOT most VRE
Protein Synthesis Inhibitors
These target the bacterial ribosome (70S vs 80S).
- macrolides
- aminoglycosides
- lincosamides
- tetracyclines
- other
Macrolides have a broad spectrum of activity. They are bacteriostatic, with time dependent killing.
These bind the 50S subunit.
erythromycin
coverage |
indications |
adverse effects |
Gram positive
NOT
Gram negative
|
second line
|
|
clarithromycin (Biaxin)
coverage |
indications |
adverse effects |
|
once daily drug RTI, skin infections, mycobacteria, H.pylori |
azithromycin (Zithromax)
coverage |
indications |
adverse effects |
|
first line for chlamydia may also be used for:
|
|
Aminoglycosides
Aminoglycosides are excellent for gram-negatives. They are bactericidal, killing in a concentration-dependent manner. Irreversibly bind 30S subunit. Do not work against anaerobes, as they require oxygen-dependent influx.
Drugs include: gentamycin, tobramycin, amikacin, neomycin, streptomycin.
coverage |
indications |
adverse effects/comments |
gram negative
|
|
|
Once daily dosing is more effective and less nephrotoxic and ototoxic. Connventional dosing is done with pregnancy, ascites, cystic fibrosis, burns, and renal failure.
Streptomycin
- used in conjunction with other agents in the treatment of M tuberculosis
- also has activity against M leprae, Y pestis, and others
lincosamides
irreversibly binds the 50S subunit, inhibiting protein initiation
clindamycin
coverage |
indications |
adverse effects and notes |
gram positives
Not
|
anaerobic infections, usually with anti-GN
|
|
Tetracyclines
Members include tetracycline, doxycycline, minocycline. Main mechanism of resistance is efflux.
coverage |
indications |
adverse effects |
gram positives
common gram negatives
atypicals (excellent)
B. burgdorferi
poor:
|
|
|
tigecycline.
glycylcycline. derivative of monicycline.
IV; poor oral bioavailability.
coverage |
indications |
adverse effects |
gram positives
|
|
|
daptomycin (where should this go?)
cyclic lipopeptide. Bactericidal; concentration-dependent killing. Irreversibly binds to bacterial cell membrane, forming a pore that leads to rapid depolarization through K efflux
coverage |
indications |
adverse effects |
Corynebacterium jeikeium Enterococcis Staphylococcus epidermidis
|
Other
chloramphenicol
inhibits protein synthesis by binding the 50S ribosomal subunit
coverage |
indications |
adverse effects |
|
Typhoid fever
serious infections when suitable alternatives not available |
|
oxazolidinone - inhibits initiaition of bacterial protein synthesis. Alternative to vancomycin for MRSA and VRE.
coverage |
indications |
adverse effects |
|
VRE, MRSA as outpatient |
|
daptomycin
- will be good for penetrating biofilms
DNA Synthesis Inhibitors
- fluoroquinolones
- other
Fluroquinolones
Fluoroquinolones act on DNA gyrase and topoisomerase IV, causing permanent DNA double-stranded breaks and bacterial death.
They demonstrate concentration dependent killing. Bad for children, as DNA is important to them.
Resistance can occur with DNA gyrase mutations, cellular membrane efflux, and decreased porins.
They have excellent bioavialability, though concentration is lower in the CSF. They are predominantly renally excreted, causing concentration in urine, but requiring dose adjustment.
ciprofloxacin, norfloxacin, ofloxacin
coverage |
indications |
adverse effects/comments |
gram positives -
gram negatives +++
|
use only when necessary to prevent resistance
|
|
levofloxacin, moxifloxacin
coverage |
indications |
adverse effects/comments |
gram positives ++
gram negatives +++
|
|
|
Other
metronidazole (Flagyl)
Leads to free radical release, damaging DNA and other macromolecules. First needs to be reduced. Good oral viability.
coverage |
indications |
adverse effects |
anaerobes
poor
|
|
|
Rifampin
inhibits RNA polymerase, preventing RNA synthesis. It cannot be used alone due to rapid development of
coverage |
indications |
adverse effects |
|
|
|
Metabolic Pathway Inhibitors
Trimethoprim/sulfamethoxazole (TMP/SMX) blocks folic acid synthesis at two steps; bacteria cannot obtain folate from their environment and rely on its synthesis to proliferate. Resistance if organism can bypass metabolic requirements. Good CNS penetration
coverage |
indications |
adverse effects |
|
UTR, RTI, GI infections, skin and soft tissue, PCP |
|
nitrofurantoin (MacroBID, Macrodantin)
coverage |
indications |
adverse effects |
poor against:
|
lower UTI; not pyelonephritis or bacteremia |
|
Antimycobacterials
Always used as combination therapy (minimum three) due to high rates of resistance.
These drugs are given over a long duration, ie 6 months or more.
drugs |
coverage |
indications |
adverse effects |
|
|
|
inhibits formation of the mycobacterial cell wall |
|
rifampin
|
|
active TB, other mycobacterial infections; prosthetic endocarditis |
|
ethambutol |
|
|
|
pyrazinamide |
|
||
sulfones |
|
||
clofazimine |
|
History of Antibiotic Development
SPICE
AmpC inducible; resistant to third-generation cephalosporins.
- Serratia
- Pseudomonas
- Indole positive
- Citrobacter
- Enterobacter
Can use:
- carbapenems
- vancomycin
- etc
Antibiotic Resistance
Bacterial reistance to antibiotics may be innate (ie with Pseudomonas) or acquired, either through mutation or transformation/congulation of foreign DNA.
Resistance is increased by:
- inadequate levels of antibiotic at site of infection
- too short a treatment time
- elevate numbers of organism
- overuse of antibiotics
- frequent exposure to the same class of antibiotic
General mechanisms of resistance:
- altered permeability
- inactivation/destruction of antibiotic
- altered drug binding site
- new binding sites
- drug pumps
- bypass of metabolic pathways
Erythromycin can turn on resistance to clindamycin in some bacteria.
An antibiogram is an antiotic susceptibility chart.
Antibiotic Allergy
Many people are not clear regarding allergy.
Immunologically mediated reactions include:
- reaction does not resemble the drug's pharmacologic effect
- lag time to reaction
- reaction may occur with minute doses
- symptoms characteristic of allergic reaction (hives, bronchospasm, etc)
- reaction resolves after drug is discontinued
- reaction is preproduced by agents with similar chemical structures
Penicillin
Approx 10% of patients in one study reported being allergic to penicillin, while 90% of these people are able to tolerate penicillin (Khan et al, 2010).
Up to 20% of the hospitalized population believes they are allergic to penicillin. However, in patients with an anaphylactic response, only 20% are still allergic after 10 years.
Cross-reactivity to cephalosporins, which have a similar penicillin ring, is very controversial. If any concern, use 2nd or 3rd generation cephalosporins.
Resources and References
Khan DA et al. 2010. Drug Allergy. J Allergy Clin Immunol. 125:S126-7.
McLean-Toole A et al. 2011. Practical management of antibiotic allergy in adults. J Clin Pathol. 64:192-199.
 |