
Atherosclerosis and Ischemic Heart Disease
last authored: Jan 2010, David LaPierre
last reviewed:
Introduction
Athersclerosis ("a hardening of the arteries") is the progressive accumulation of lipids, smooth muscle cells, connective tissue, leukocytes, and platelets inside the intima of arterial walls.
They develop primarily in elastic arteries such as the aorta, carotid, and iliac arteries and large/medium muscular arteries such as the coronary or popliteal arteries.
Atherosclerosis is the leading cause of death in most developed countries.
Atherosclerosis starts early - almost 20% of people under 20 have arterial accumulations, while over 85% of people over 50 do.
The Case of...
a simple case introducing clincial presentation and calling for a differential diagnosis to get students thinking.
Causes and Risk Factors
Risk factors include:
- hypertension
- smoking
- diabetes
- high plasma LDL and low HDL
- elevated plasma triglycerides
- family history and genetic polymorphisms
- infection and inflammation
- metabolic syndrome
- homocysteine
Hyaline athersclerosis is associated with hypertension and is more prevalent and severe in people with diabetes.
Ischemic heart disease results from an imbalance between perfusion (supply) and workload (demand) of the heart. Ischemia not only involves oxygen insufficiency, but also reduced nutrient concentration and inadequate removal of metabolites.
In more than 90% of cases, ischemia is due to atherosclerosis. For this reason, ischemic heart disease is often termed coronary artery disease.
Risk of developing IHD depends on number, distribution, and size of plaques.
Pathophysiology
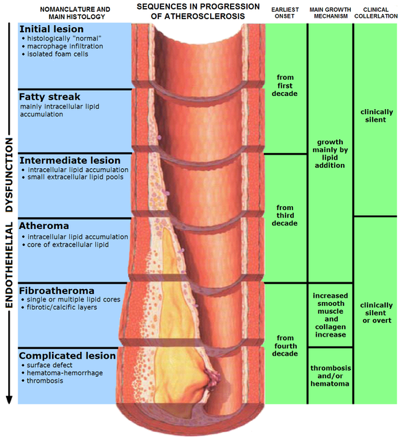
Atheromas develop over time. The American Heart Association had named six stages of progression:
- type I: isolated foam cells
- type II: fatty streak, with mainly intracellular lipid accumulation
- type III: small extracellular lipid pool
- type IV: atheroma formation, withextracellular lipid core
- type V: fibroatheroma, with fibrotic tissue and potential calcification
- type IV: complicated surface, with hemorrhage or thrombus formation
Fatty streaks are the earliest manifestation of atherosclerosis and are caused by lipid-filled foam cells. They also contain T lymphocytes. They are not significantly raised and do not cause any disturbance in blood flow.
They appear in some children below one year of age and all children 10 years of age and up, regardless of of race or environment.
Some fatty streaks may become atherosclerotic plaques, but most do not.
Plaques are dynamic, contributing to their propensity to disruption. Those containing large areas of foam cells and lipids, those with thin fibrous caps, and those with clusters of inflammatory cells are called vulnerable plaques.
The fibrous cap can undergo continuous remodeling. Levels of collagen, the major structural component, determine stability.
Atherosclerosis begins in childhood. Clinically significant plaques tend to be present eithin the first several centimeters of the LAD and LCX and along the entire length of the RCA. On occasion, the major secondary epicardial branches are involved - the diagonal branches of the LAD, obtuse marginal branches of the LCX, or posterior descending branch of the RCA.
IHD can be increased by cardiac hypertrophy, diminished oxygen supply (anemia, shock, etc), or with increased heart rate.
Athrosclerotic narrowing of the epicardial coronary arteries, together with thrombosis, platelet aggregation, and vasospasm, all contribute to IHD.
Within seconds, aerobic glycolysis stops and lactic acid begins to breakdown. A striking loss of contractility occurs within 60 seconds of ischemia onset, which can precipitate heart failure long before infarction. Only severe ischemia lasting 20-40 minutes leads to cell death, however.
Signs and Symptoms
- history
- physical exam
History
Symptomatic atherosclerosis most often involves arteries supplying heart, brain, kidneys, and lower extremities.
A fixed obstruction of coronary arteries will generally cause symptoms with exercise, while a 90% stenosis will lead to symptoms at rest.
Ischemic heart disease can appear in four ways:
acute coronary syndromes, such as myocardial infarction
chronic IHD and heart failure
Major consequences include angina and myocardial infarction, stroke, aortic aneurysms, and perihperal vascular disease (ie gangrene of the legs or arterial ulcers).
Physical Exam
Ankle/Brachial Index (ABI) is derived from (ankle systolic pressure) / (brachial systolic pressure) and measures limb perfusion.
- 1.25 suspected arterial calcification
- 0.97 - 1.25 normal
- 0.75 - 0.96 mild ischemia
- 0.50 - 0.75 moderate ischemia
- 0.35 - 0.50 moderately severe ischemia
- less than 0.35 severe ischemia
Stethescopes may be used, but Doppler is more sensitive.
Investigations
- lab investigations
- diagnostic imaging
Lab Investigations
Diagnostic Imaging
Differential Diagnosis
Treatments
Consequences and Course
The Case of...
Case #2 - a small story wrapping it all up and asking especially about management.
Additional Resources
any good free online resources for further reading.
Topic Development
created:
authors:
editors:
reviewers:
 |