
Chlamydia trachomatis
last authored: March 2010, David LaPierre
last reviewed: Nov 2011, Nadine Stevenson
Introduction
Chlamydia trachomatis is the most common sexually transmitted bacterial infection, chlamydia. Women are frequently asymptomatic, though can develop cervicitis, urethritis, and pelvic inflammatory disease, the latter causing serious reproductive conditions. In men, infection often causes urethritis, though they may also be asymptomatic.

It is also the leading preventable cause of blindness in the world - a chronic conjunctivits called trachoma. The WHO aims to eliminate trachoma worldwide by 2020.
Chlamydia is classified as bacteria, but is atypical due to its obligatory intracellular replication and lack of peptidoglycan cell wall. Other members of genus are C. pneumoniae and C. psittaci.
The Case of Sam West
Sam is a 24 year-old woman whose sexual partner tells her he has just been diagnosed with chlamydia. She is surpised, as she is asymptomatic.
- Should she be concerned?
- What investigations should be done?
- What treatments, if any, should she have?
Epidemiology
C trachomatis is thought to be the most common bacterial STI in the US, causing over 4,000,000 infections yearly. Humans are the only reservior. Approximately 5% of the general population and 20% of people attending STI clinics are infected.
Trachoma affects over 500 million people worldwide, leading to blindness in 7-9 million. It is endemic in the Middle East, North Africa, and India. Prevention of reinfection focuses on household hygiene.
C trachomatis is also the most common cause of neonatal conjunctivitis in North America.
Classification and Characteristics
C. trachomatis are round cells 0.3-1 um in diameter. They have an outer membrane containing lipopolysaccharide, but lack peptidoglycan between their two membrane layers.
These organisms are energy parasites, unable to grow outside eukaryotic cells and depending on host's high energy phosphate bonds.
C. trachomatis has two biovars, with 15 serovars (serologic variants) based upon outer membrane proteins.
- A,B,C cause trachoma
- D-K cause urethritis and cervicitis
- L causes lymphogranuloma venereum
The replication cycle of C. trachomatis begins with an infectious elementary body (EB), which is the extracellular, infective form of chlamydia. This leads to the larger intracellular reticulate body (RB), which reproduces by binary fission and depends on host cells for metabolism.
Transmission and Infection
Genital infection
The attack rate for female-to-male transmission is 30%, with an incubation period of 2-6 weeks.
C. trachomatis has an affinity for epithelial cells of the cervix, upper genital tract in women, urethra, rectum, and conjunctiva. L serovar can also gain access through minute lesions or lacerations to lead to granuloma formation.
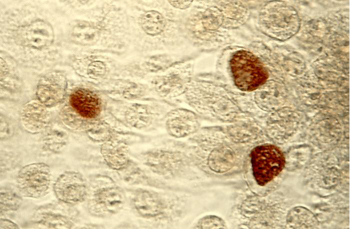
Chlamydia inclusion bodies, courtsey of PHIL #3802
C. trachomatis elementary bodies (EBs) enter cells via receptor-mediated endocytosis. Receptors for are restricted to nonciliated columnar, cuboidal, or transitional epithelium. Within the endocytic vacuole, conversion to the replicative RB occurs. Lysosomal fusion is inhibited, allowing survival in inclusion bodies (see image). Fusion with the Golgi apparatus follows, forming a large inclusion body. After 48-72 hours, the process reverses and multiple EBs form, are released from the host cell, and go on to infect other neighbouring cells.
Epithelial cells release IL-8 and other cytokines in response to LPS and infection. This leads to influx of neutrophils, lymphocytes, macrophages, and B cells. Ongoing infection can lead to necrosis, fibrosis, and scarring.
Immunity is uncommon, though IgA may attenuate genital infection.
Conjunctival infection
Trachoma is transmitted by eye-to-eye by droplets, hands, clothing, and flies. Young children are the most common reservoir. It may also be transmitted by respiratory droplet or fecal-oral route. Persistent or recurrent infections, along with host immune response, leads to scarring and blindness.
Clinical Manifesations
Genital infection
Up to 40-60% of people infected with chlaymdia are asymptomatic, with women more commonly affected.

Chlamydia cervicitis, courtesy of PHIL (#3795)
In women, symptoms can be similar to those of Neisseria gonorrhoeae, with urethritis characterized by dysuria and a thin urethral discharge. Cervicitis can lead to vaginal discharge, but is usually asymptomatic. Salphingitis/pelvic inflammatory disease occurs in 5-30% of women, potentially leading to sterility or ectopic pregnancy.
Urethritis and epididymitis can occur in men, causing pain and discharge.
Infection does not cause long-lasting immunity; instead, re-infection results in acute inflammation and tissue damage. Vision loss and sterility can result.
Eye infection
Trachoma is characterized by chronic conjunctivitis and scarring. It causes follicular conjunctivitis, with inward-turning eyelids and corneal ulceration and scarring. Visual loss can occur 15-20 years after initial infection.
Inclusion conjunctivitis occurs 5-12 days after birth and is characterized by watery, then mucopurulent discharge. It follows vaginal birth in 1/3 of infected mothers. Prophylaxis is not helpful. Untreated infection can last 3-12 months. Adults may also develop conjunctivitis from C trachomatis strains associated with STIs.
The WHO has created a trachoma scoring card (outside link).
Other
LGV (lymphogranuloma venereum) begins with a small, painless lesion and is marked by serious inflammation and multilocilar lymph node swelling. Progression can lead to matted, suppurative bubos. Systemic symptoms can include fever, headaches, chills, arthalgias, and myalgias.
Interstitial pneumonia can develop in infants, with difficulty feeding, dyspnea, and a pertussis-like cough.
Diagnosis
Epithelial cells are required for detection, as C. trachomatis is intracellular. For females, cervical swabs are preferred, while urethral scrapings are best for males.
Urine is an effective sample for polymerase chain reaction (PCR) detection. Nonculture methods include:
- direct fluorescence antibody visualization against elementary bodies
- enzyme immunoassay against chlamydial lipopolysaccharide
- nucleic acid amplification (NAA), including PCR, frequently using a common plasmid sequence
Culture is 70-80% sensitive and involves antimetabolite-treated cell lines to prevent host cell replication but allow C. trachomatis to grow. Cells are stained using fluorescence or iodine.
Serology is of limited value because titres persist for a long time following infection.
Diagnosis of inclusion conjunctivitis can be made with smears of conjunctival scrapings, followed by immunofluoresence, culture, or PCR.
Treatment
C. trachomatis is sensitive to tetracyclines, macrolides, and some fluoroquinolones.
Azithromycin is first-line for STI and given as a single oral dose. Amoxicillin or erythromycin are used in pregnant women.
Trachoma can also be treated with a single dose of azithromycin or 14 days of a tetracycline. Surgery is required for severe corneal or conjunctival scarring.
Prophylactic ocular antibiotics are frequently given routinely to neonates. Infants born to infected mothers should receive systemic treatment to prevent inclusion conjunctivitis, pneumonia, or seeding of the vagina and rectum.
Resources and References
Centre for Disease Control (CDC) Chlamydia resources
World Health Organization - Trachoma
 |