
Prenatal Abdominal Exam
last authored: Aug 2011, David LaPierre
last reviewed: Oct 2011, Dax Biondi
Introduction
Much information can be gained by measurement and palpation of the pregnant abdomen, including fetal growth and presentation. As these exams require no equipment other than a measuring tape, they are very helpful in any setting. However, they also require much experience in order to develop the skill necessary to provide reliable information.
There are a number of terms used to describe how the fetus is sitting within the uterus, in relation to the pelvis.
Lie: the orientation of the infant to the mother. May be longitudinal (99% at birth) or transverse.
Presentation: the part of the fetus that is closest to the birth canal. In longitudinal lie, presentation may be cephalic (head first - this is the most common presenting part) or breech. There are three types of breech presentations. Frank Breech positioning accounts for 50-75% of breech presentations; the baby's hips are flexed and knees are extended. Footling or Incomplete Breech accounts for 20% of breech presentations; the baby is extended at both the hips and knees. Finally, Complete Breech accounts for 5-10% of breech presentations; both the baby's hips and knees are flexed and the baby's feet are above the buttocks. With transverse lie, the shoulder is the usual presenting part.
Position: the fetal part that is presenting to the birth canal: occiput, chin (mentum), sacrum, or acromion.
- occiput anterior (OA); also left/right occiput anterior (LOA/ROA)
- occiput posterior (OP); also left/right occiput posterior (LOP, ROP)
- occiput transverse left/right (LOT, ROT)
Symphysis to Fundal Height
Symphysis to Fundal Height (SFH) gives a reasonable assessment of the size of the uterus and after 20 weeks gestation, approximates gestational age in weeks (that is, at 20 weeks gestation, SFH should equal twenty centimetres plus or minus two
12 weeks: fundus at pubic symphysis
20 weeks: fundus at umbilicus
27 weeks: fundus at sternum
centimetres). It requires minimal equipment, though can present a challenge when obesity is present. It is measured from the top of the symphysis pubis to the top of the uterus. It is encouraged that the person performing the measurement not look at the length as it is measured but rather, mark the length roughly with the fingers over the fundus, remove the tape measure and read the measure once off the abdomen. Otherwise, it is tempting to adjust your estimate of the location of the fundus to suite your knowledge of the known gestational age.
Large fundal height can occur with:
- multiple pregnancies
- inacurate dates
- diabetes (fetal macrosomia)
- fibroids
- large parents
- polyhydramnios
Modified Leopold's Maneuvers
Modified Leopold's maneuvers are used to assess fetal presentation and position during the last few months of pregnancy and during labour (between contractions). They are not relevant under 34 weeks, as the baby will be freely moving. After this time, the fetus tends to remain in one position.
Experienced examiners can identify fetal malpresentation with high sensitivity and specificity (Lyndon-Rochelle et al, 1993), but the exam can be challenging or impossible if the mother is obese, if there is polyhydramnios, or if the placenta is anterior.
The mother should lie on her back with her abdomen exposed. There are four maneuvers to perform:
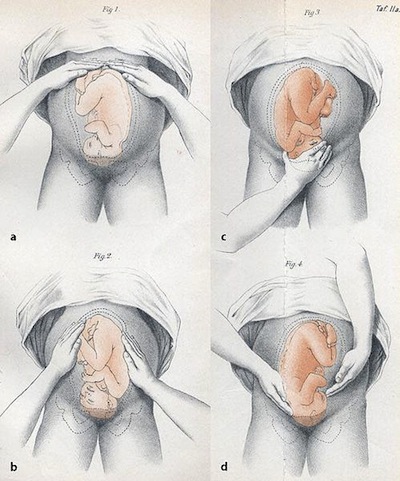
Leopold's maneuvers, Christian Gerhard Leopold, 1894
1: Standing facing the mother's head, with fingers together and using the pads of the finger tips of both hands, gently palpate the uterine fundus and determine what occupies it (head, limb or buttocks). Most commonly, the buttocks may be found here; it feels less globular than the fetal head.
2. Next, place one hand on each side of the maternal abdomen. Use one hand to steady the uterus and the other to palpate the fetus. Gently switch these roles from hand to hand. The hand on the back feels a long, smooth length, the length of the hand or longer. The other hand will feel the irregular surface of the fetal limbs and perhaps a kick if the fetus is awake and active.
3. Now, turn to face the maternal feet. The next objective is to assess if the presenting part has descended into the pelvis. With finger tips together and the finger tips of the left and right hand initially in contact, palpate the area just above the symphysis pubis. Apply gentle downward pressure and note whether the hands stay together or are forced apart as you attempt to push your fingers posterior, above the symphysis pubis. If the hands can stay together with suprapubic pressure, this suggests the presenting part is not yet engaged.
4. Further assess the presenting part. With you dominant hand, firmly grasp the presenting part in the lower pole of the uterus. With your non-dominant hend, apply gentle downward pressure from the uterine fundus simultaneously. If the presenting part is not engaged and the presentation is vertex, you should be able to move the head independently of the rest of the body.
Resources and References
Lyndon-Rochelle et al. 1993. Accuracy of Leopold's maneuvers in screening for malpresentation: a prospective study. Birth. 20:132.
 |