
Giardia lamblia
last authored: March 2010, David LaPierre
last reviewed:
Introduction
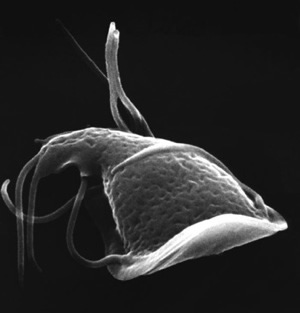
Giardia lamblia (synonyms: Giardia duodenalis, and Giardia intestinalis) is a protozoan flagellate parasite found around the world.

Giardia about to settle on intestinal wall
courtesy of CDC, PHIL #11642
Infection can follow ingestion of Giardia cysts in contaminated water or food, or via the fecal-oral route. Intestinal infection can be asymptomatic, though it commonly causes acute gastrointestinal symptoms (giardiasis, or beaver fever) such as nausea, vomiting, and diarrhea.
Disease is normally self-limiting, though chronic infection can also occur.
Giardia is a flagellate whose shape is determined by a rigid cell wall (unlike amoebas).
Giardia, courtesy of CDC PHIL #11624
The Case of Riza Deware
Riza Deware is a 34 year-old woman living in rural Canada. She goes camping and drinks some water from the lake they are camping beside. Ten days later, she develops nausea, vomiting, abdominal pain, and diarrhea.
She goes to her family doctor, who suspects giardiasis and sends a stool sample to the lab.
What is he looking for in the stool?
Epidemiology
Giardia is found worldwide, but is more prevalent in warm climates, and in children. People can act as carriers for the disease.
Infectious cysts may be found in water, food, or passed person-to-person through the fecal-oral route. Contaminated water sources include wells ponds, lakes, and streams. They may also occur in city reservoirs, as cysts are resistant to water treatment. Giardia is the leading cause of infectious waterborne diarrhea outbreaks in the United States (EPA).
Lifecycle, Transmission, and Infection
Cysts are resistant forms and are responsible for transmission of giardiasis. The cysts are hardy and can survive several months in cold water.
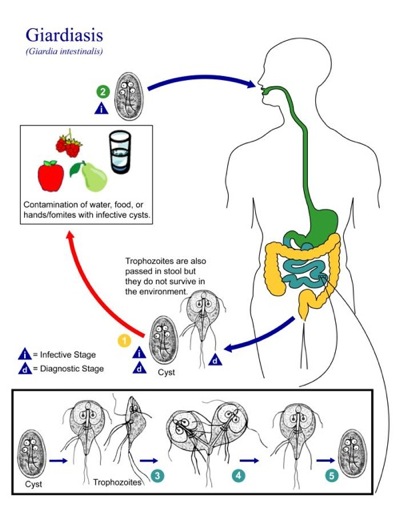
Giardia lifecycle, courtesy of CDC PHIL #3394
Infection occurs by the ingestion of cysts in contaminated water, food, or by the fecal-oral route (hands or fomites).
In the small intestine, each cyst releases two trophozoites, which absorb their nutrients from the lumen of the small intestine, and are anaerobes.
Trophozoites multiply by longitudinal binary fission, remaining in the lumen of the proximal small bowel where they can be free or attached to the mucosa by a ventral sucking disk. IgA blocks attachment to intestinal wall.
Encystation occurs as the parasites transit toward the colon. The cyst is the stage found most commonly in nondiarrheal feces.
Because the cysts are infectious when passed in the stool or shortly afterward, person-to-person transmission is possible. While animals are infected with Giardia species, their importance as a reservoir is unclear.
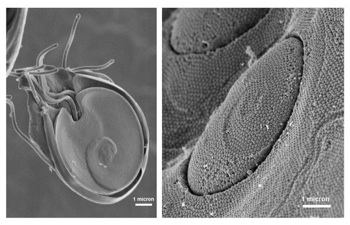
courtesy of CDC, PHIL#11644
They adhere to the instestinal wall, as shown in the accopmanying image. Colonization of the gut results in inflammation and villous atrophy, reducing the gut's absorptive capability.
The parasites are not tissue invasive, and do not cause any systemic disease.
Clinical Manifestations
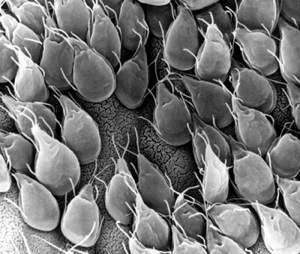
courtesy of CDC, PHIL#11632
Giardia infections can remain asymptomatic, though they can also result in acute or chronic diarrhea, which may be severe.
Acute giardiasis develops after an incubation period of 1-14 days and usually lasts 1-3 weeks. Symptoms include diarrhea, abdominal pain, anorexia, bloating, nausea, and vomiting.
In chronic giardiasis, symptoms are recurrent and can lead to failure to thrive, malabsorption and debilitation.
Diagnosis
Giardiasis is diagnosed by the identification of cysts or trophozoites in the feces, using direct mounts as well as concentration procedures. Repeated samplings may be necessary, and three negative tests should be carried out before declaring a patient negative. Because trophozoites break down quickly, stool samples should be in preservative or fixative such as SAF or PVA. To maximize recovery of cysts, stool samples should be concentrated prior to microscopic examination.
In bright-field microscopy, cysts appear ovoid to ellipsoid in shape and usually measure 11 to 14 μm (range: 8 to 19 μm). Immature and mature cysts have 2 and 4 nuclei, respectively. Intracytoplasmic fibrils are visible in cysts. Stained trophozoites (i.e., using trichrome or iron hematoxylin) appear as pear-shaped organisms, measuring 10 to 20 μm. Trophozoites have two anteriorly placed nuclei and 8 flagella, though flagella are rarely seen. Trophozoites are often described as looking like a face. (outside link: CDC microscopy)
Other techniques include enzyme immunoassays and immunofluorescence. Lastly, duodenal fluid or duodenal biopsy may be done, if necessary, to demonstrate trophozoites.
Treatment
Several prescription drugs are available to treat giardiasis including metronidazole and tinidazole. Nitazoxanide appears effective in children.
Resources and References
Center for Disease Control, DPDx
Environmental Protection Agency (EPA)
 |