
Filtration and Excretion in the Kidney
last authored:
last reviewed:
Introduction
The kidney receives one fifth of the body's blood flow and filters about 25% of that.
While the kidney filters about 180L/day, it excretes only 1.5L daily, reabsorbing over 99%.
Filtrate is almost identical to plasma without its plasma proteins, with an osmolarity of 300 mOsM.
- glomerular filtration rate
- tubular function
- waste excretion
Glomerular Filtration Rate
GFR is dependent on renal blood flow, resistance to flow, and glomerular permeability. Normal GFR is about 100ml/min for women and 120 ml/min for men, but increases during pregnancy. It depends on body size, age diet, and physiologic state. Measuring GFR is a key indicator of kidney function.
When arterial pressure increases, afferent resistance increases, while efferent resistance decreases.
Modulation of afferent and efferent arteriolar pressure, as well as filtration surface area by mesangial cells, controls filtration rate.
The macula densa also senses NaCl concentration, linked with increased flow, and provides feedback to the GFR apparatus, with increased [NaCl] inducing a drop in GFR.
Intrinsic arteriolar autoregulation, the myogenic response, controls flow based on blood pressure. Autoregulation can be intefered with with age or with ACE inhibitors.
Reductions in GFR is a hallmark of renal disease. Changes can include reduction in number of nephrons in chronic renal disease, reduction in glomerular perfusion in afferent arteriolar resistance, or obstruction to urinary outflow.
Prostaglandins act on arterioles, the afferent more than the efferent to cause vasodilation and increase GFR. Angiotensin II is a vasoconstrictor under control of renin. It also acts to increase GFR.
Norepinephrine is released to increase BP and prostaglandin release. Dopamine is another vasodilator. ANP is an afferent vasodilator and an efferent vasoconstrictor.
Factors dilating the afferent arteriole, increasing GFR:
- prostaglandins
- kinins
- DA: opposes NE action
- ANP: hemodynamic effects
- NO: vasoconstrictor
- Ang II low dose (actually constricts efferent arteriole)
Factors constricting the afferent arteriole, decreasing GFR:
- Ang II high dose
- norepineprine and epinephrine: restricts both RBF and GFR
- endothelin
- adenosine
- ADH: facilitates water retention
- PG blockade
Tubulo-glomerular feedback causes a decrease in GFR with increased nephron perfusion rate. This appears to involve the macula densa and chloride.
Changes in GFR are the hallmark of renal disease. These changes include reduced numbers of nephrons, reduced glomerular perfusion, or obstruction of urinary outflow.
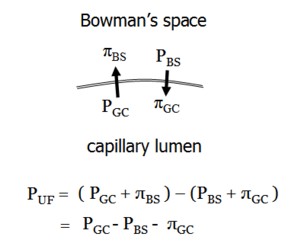
At the beginning of the capillary, the hydrostatic pressure in the capillary forces water and solutes out. As the fluid moves through the capillary, oncotic pressure increases such that net filtration decreases. Normally filtration is still occuring at the end of the capillary, but wilth low RBF some of the capillary is 'wasted' as filtration equilibrium is reached.
Tubular Function
Following production of ultrafiltrate, the tubule system regulates fluid and electrolyte perturbations due to diet and metabolism in a number of ways.
Net absorption occurs of sodium, chloride, water, bicarbonate, glucose, amino acids, phosphates, calcium, magnesium, uric acids and others. Secretion of hydrogen ions, ammonium ions, and a large number of organic acids and bases also occurs. Urea and potassium undergo both absorption and secretion, depending on the circumstance. The multiple roles of the tubule is accounted for by the diversity of its cells.
The Proximal Tubule
The proximal tubule reabsorbs isotonically about 60% of filtered Na+, Cl-, K+, water, and urea, as well as 90% of the filtered bicarbonate.
A large brush border at the lumenal membrane enables large transepithelial mass flow. Junctional complexes join proximal tubule cells at their apex, forming a leaky epithelium which allows water and solute passage.
Almost all filtered glucose and amino acids are reabsorbed here as well. Phosphates are reabsorbed, significantly affected by PTH action.
The primary mechanisms of transport are linked to Na.
Protons are excreted using the Na/H exchanger, regulated by cAMP. Na flows out of the cell via the Na/K exchanger and the Na/HCO3- symporter.
In the straight portion of the proximal tubule, organic acids and drugs are secreted.
Ammonia synthesis also occurs in the proximal tubule.
Loop of Henle
The descending loop of Henle is water permeable, while the ascending limb is impermeable. This leads the medullary interstitium to become quite hypertonic, creating an osmotic gradient that pulls water from the descending limb and collecting duct.
Passive water absorption occurs in the thin descending limb, while salt absorption occurs in the thin ascending limb. About 15% of ultrafiltrate and 25% of NaCl is reabsorbed, creating a dilute solute entering the distal tubule.
The thick ascending limb actively absorbs NaCl using an Na-K-2Cl cotransporter. K+ entering the cell is recycled at the lumen via a K+ channel. This maintains co-transporter activity, enables K+ secretion, and allows paracellular cationic absorption. Loop diuretics such as furosemide are potent inhibitors of the co-transporter.
Movement of NaCl from the thick ascending limb to the interstitium creates hypertonicity that allows water absorption from the thin descending limb and the collecting ducts during dehydration.
Collecting Duct
The collecting duct is crucial to achieving salt and water homeostasis. During volume depletion, aldosterone renders the urine virtually free of Na+. The cortical collecting duct is composed of both principal and intercalated cells, while the latter are absent in the medulla.
Intercalated cells are important in acid-base homeostasis, rather than Na and K regulation.
Waste Excretion
The kidney is responsible for eliminating nitrogenous wastes produced by protein catabolism. These wastes are filtered at the glomerulus. As their plasma concentration must be low to maintain homeostasis, large volumes of ultrafiltrate pass through the kidney.
Many toxins, such as organic acids (lactate, urate, etc), bases (ie morphine) and many xenobiotics can also be secreted through the proximal tubule. This is the major mechanism for toxins that are protein-bound.
 |